 Tweet
Tweet
Is both weird and logical, isn't it? But it's consistent. This is a generalization, but theirs is a highly permissive but exclusive society, whereas ours is not permissive but more inclusive.
-
-
There's also much less fiscal conservatism. LePen has proposed lowering the retirement age and expanding benefits. It's not clear to me that a ton of French people would worry about how she'll pay for it.Comment
-
Right. Nationalism doesn't have to be conservative.Dan Patrick: What was your reaction to [Urban Meyer being hired]?
Brady Hoke: You know.....not....good.Comment
-
People are talking like Dearborn is something foreign. Trust me, you guys would be safe going to Dearborn. Plus there is kind of a misconception as a lot of people don't know the difference between Chaldeans and Muslims. Hamtramck has more of a Muslim to tinge along with old Polish ladies.Comment
-
I'm not talking about Dearborn as foreign. My assumption is that it is a great example of an American-Muslim community.Dan Patrick: What was your reaction to [Urban Meyer being hired]?
Brady Hoke: You know.....not....good.Comment
-
Dearborn is great. One aspect of assimilation that should be more appreciated is that you can get a mixed-kebab platter on which the meat is not overcooked. And that white-garlic sauce is another example of assimilation. That stuff is brilliant, but it was invented here, because Americans were accustomed to tzatziki with their gyros/doner. More assimilation.Comment
-
Like I said about the difference between Chaldeans and Muslims, big difference. It's more correct to talk about Arab-Americans as opposed to Muslim-Americans when referring to Dearborn. Although I'm not sure that a Renaissance Man like Steve King really cares about the distinction.Comment
-
Jeff. Thanks for the thoughtful reply.
I particularly like the idea of those Integrated Practice Units. I play golf with a Chiropractor who often says that there should be one-stop shopping for back pain where health care nerve guys, bone guys, back guys, chiropractors, acupuncturists, and psychologists are in one place where they consult on each patient. He has a saying "....if all you have is a hammer, everything looks like a nail."
IPUs also have the potential to be large enough players in the health markets to allow them to negotiate lower prices for drugs and services. Free market guys like myself like this kind of countervailing power.
I also think there is an element of tort reform needed in any health care overhaul. All you need to do is watch TV and you see ads for all sorts of "class action" lawyers looking for victims. Next thing you know, talcum powder will have to have a skull and crossbones on each bottle. I think IPU physicians might monitor their colleagues if liability insurance covers the whole IPU and not the individual provider.Comment
-
the key to any medical cost containment is containing overkill by using common sense--so much of what PCP's and GP's used to do is pharmed out to specialists at a drop of a hat.
No matter what you are admitted to the hospital for you can count on a variety of specialist circling your bed especially if you have good insurance
knowing when to pull the plug on medical care is another essential part
so much is fear of legalities by those who overkill but most is straight profit.
until we come up with a way to discourage overkill by the systems out to make profits medical care as a business will continue to eat away at everyone's checkbook
the other aspect I've seen is a drastic increase in offices who manage health. what used to consist of AA and a few others has mushroomed into lots of offices with varying amounts of assistant this and quality that and risk this and accredidation that--providers are shoehorned into sharing offices where I work while the administrative chief o risk stratification and quality control and his 3 assistants occupy what used tobe a full time thriving clinic.
so now I know the urge for slivovitz talent and AA's roots
mine are from the 1890's one of those krauts somebody referenced earlier came over and great grandpa actually fought ww1 and grandpa fought in ww2 against those same krauts. I think being good catholic krauts we rep[roduced and now my namesake from my great grandpa he had 6 kids my grandpa had 5 and my dad had 5--I stopped at 3. now have 3 from oldes boy. I must be one of about 150 descendants from the original crash who came over in the 1890'sComment
-
I've said here many times that I favor unlimited legal immigration. Legal immigrants are not allowed "social services"-type welfare for five years, and an actual human has to take the responsibility for their financial support.
Willingness to assimilate is the touchstone of any immigration policy. We all implicitly know this. My Dutch grandparents did not allow their children to speak Dutch in the home, and they made a point of learning English as quickly as they could.
In the US, English is the language of commerce. Unless you are on some form of government assistance, proficiency in English is necessary to economic well-being. I take two things away from this.
1. Immigrants should not be eligible for any government assistance for a period of 5 years; this includes illegal immigrants. This is now the law.
2. Speaking English is not only the first step toward assimilation for newly arrived immigrants, and it is a necessary pre-condition for upward mobility for following generations. Why then do we (in the US) allow or require Spanish-translation in virtually every form of commercial/governmental interaction? The US needs to be less accommodative of foreign languages. The language you speak affects the way you think. If we want assimilation, then English-only is sound policy.Comment
-
Originally posted by SeattleLionsFan View Post
I also think it is inappropriate to enforce the law in one area and not another because it's not "politically correct".Grammar... The difference between feeling your nuts and feeling you're nuts.Comment
-
The Keckley Report March 13, 2017
The American Health Care Act: What You Need to Know and What you Need to Watch
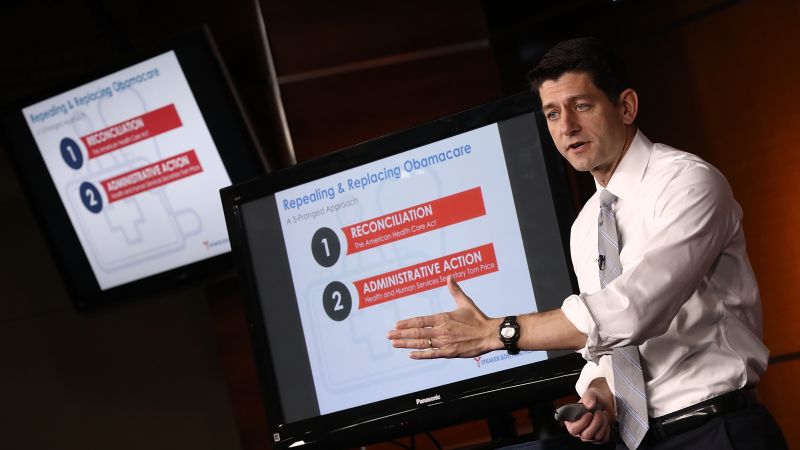
Last Monday, as promised, House Speaker Paul Ryan fulfilled his pledge to offer up the GOP’s plan to replace the Affordable Care Act.
In reality, America’s Health Care Act (AHCA) is not a new plan. Rather, it’s an updated version of the “Restoring Americans' Healthcare Freedom Reconciliation Act of 2015” that passed the 114th Congress October 23, 2015 before being vetoed by President Obama. Surrogates for this plan are quick to point out that their Repeal and Replace effort also encompasses administrative orders from HHS Secretary Tom Price, executive orders from President Trump and legislation to be passed through regular order (requiring 60 Senate votes). But the AHCA is unquestionably the first and most important of these elements: it signifies to Repeal and Replace proponents that the new Republican majority intends to make good on its promise to dismantle the Affordable Care Act.
Its status is this: the AHCA cleared the House Ways and Means and Energy and Commerce Committee votes last week. Later today, the Congressional Budget Office will render its assessment of the plan’s financial impact and its underlying assumptions about possible changes in insurance coverage. After passage in the House, it will go to the Senate where it will be modified and likely passed along party lines under the restrictions of reconciliation. Its sponsors hope it will be law within six weeks as their initial phase of Repeal and Replace.
I read the AHCA several times last week. Here’s what I concluded:
The calculus underscoring the AHCA is based on three fundamental beliefs held widely by its sponsors:
• The U.S. healthcare system is best run as a private market in which the physician-patient relationship is central. The federal government should play a limited regulatory role deferring its primary oversight to states. The public’s interest is best served by policies that promote competition with limited regulation.
• Reducing health costs is the primary aim for Repeal and Replace. Projected spending for Medicare, Medicaid, CHIP and federal employee health coupled with new Affordable Care Act-authorized costs for Medicaid expansion and subsidized coverage threatens to de-stabilize our economy, exacerbating deficits already mounting.
• The Affordable Care Act’s mandate to purchase insurance is an overreach by government and unconstitutional: it should be replaced by incentives for individuals to purchase private insurance and assume greater accountability for the costs and coverage they desire.
With these in mind, the major elements in the American Health Care Act are these:
• Insurance coverage: The primary focus of coverage is two-fold: Medicaid expansion (below) and changes to the individual market. The AHCA repeals the individual and employer mandates and penalties to purchase coverage. In 2020, it replaces the ACA’s income-based premium subsidies with tax credits adjusted for age. (Eligibility for new tax credits phases out at income levels between $75,000 and $150,000). It permits insurers to charge a late enrollment penalty (30%) for people who don’t stay continuously covered and encourages the use of Health Savings Accounts by doubling annual tax free contribution limits ($6550 for individual/$13,100 for couple) and the threshold for Flexible Savings Accounts.
• Insurance oversight: The AHCA reduces regulatory constraints over health insurers permitting them greater latitude in pricing their plans while maintaining prohibition against discriminatory premiums and pre-existing condition exclusions, extension of dependent coverage to age 26 and expansion of actuarial risk band from 3:1 to 5:1 unless states adopt different ratios (allows insurers to charge older enrollees five times as much as young and healthy). It keeps the current insurance marketplaces, open and special enrollment periods and essential health benefits requirements for qualified health plans. And it repeals the deductibility limits for highly compensated insurance executives.
• Medicaid: The AHCA suspends funding for Medicaid expansion after 2020 and encourages states to test new models for Medicaid management via a new State Innovation and Stability Program ($100 billion/10 years) to improve management of high risk individuals. It converts federal Medicaid funding to a per capita allotment beginning in 2020 using 2016 as a base year and prohibits funding for Planned Parenthood Clinics.
• Medicare: It makes no changes to Medicare benefits or Medicare Advantage. Alternative payment programs like bundled payments and accountable care organizations continue for the time being and changes to enrollee premiums for Medicare Part B and D do not change.
• Funding: The AHCA repeals excise taxes paid by insurers, drug and device companies and tanning salons along with investment taxes paid by high earners (3.8% tax on investment income and .9% income tax on individuals earning above $200,000/families above $250,000) reducing federal funding linked to the Affordable Care Act by $600 billion. It repeals funding for the Prevention and Public Health Fund at the end of FY2018 and provides supplemental funding for community health centers of $422 million for FY 2017. And it pushes the Cadillac tax on expensive employer-sponsored health plans out to 2025.
The AHCA doesn’t cover everything nor does it repeal key areas of the Affordable Care Act that address changes in the delivery system, the healthcare workforce, et al. It addresses the most politically charged issue in health reform: insurance coverage. It seeks to curtail federal obligations for Medicaid expansion by shifting its oversight to states and it changes the individual insurance market to a less regulated elective market wherein high deductible products are purchased voluntarily. (Regretfully, the spin about soaring insurance premiums, which have averaged 25% for the 12 million who purchase through health exchanges, has been portrayed as if applicable to all who are covered by private insurance. More accurately, the individual market is a small part of the private insurance market, and the restrictions around coverage through the marketplaces made it difficult for most insurers to make profit in this line of business.)
Beyond the AHCA, other legislation and administrative orders are anticipated from new leaders in Health and Human Services (Sec. Tom Price), the Veterans Administration (David Shulkin), the Food and Drug Administration (Scott Gottlieb), the Department of Justice (Attorney General Jeff Sessions) and others. So, healthcare will be prominent in news cycles and on state and federal legislative calendars for the foreseeable future. The American Health Care Act is just a start.
In its current form, the American Health Care Act makes several big bets about the future of the country’s health system:
• It bets that concessions made to the private insurance industry will result in lower premiums with suitable coverage that attracts large numbers of young, healthy, and the under-insured adults to purchase coverage voluntarily.
• It bets that tax credits will be the right hook to get large numbers of young, healthy adults to buy health insurance and premiums will be priced low and cover enough to merit their participation.
• It bets that private insurers will not exit the individual market nor abandon the health exchanges.
• It bets that older and sicker folks will be able to afford policies, since they’ll be priced higher.
• It bets that the promotion of High Deductible plans will not result in lower and middle income households being unable to afford their deductibles, resulting in delayed or neglected care.
• It bets that states will capably shoulder expanded oversight for Medicaid and insurance programs while their federal funding is cut, and it bets that the majority of the 14 million who gained coverage as a result of its expansion will not lose coverage.
• It bets that planned cuts in Medicaid and Medicare funding by the federal government coupled with increased pressures by states in their expanded Medicaid management role will not put hospitals and physicians out of business.
• And it bets that reducing the federal coffers by $600 billion as a result of the Repeal will not add to the federal deficit.
To be fair, there were big bets associated with the Affordable Care Act: in March, 2010, we asked will individuals buy coverage? Will states expand Medicaid? Will employers pay or play? And will the ACA reduce health costs? Here we go again---big bets about the future of the U.S. system.
In Kansas City last week, I asked 57 participants in the Cerner Center for Health Leadership program what they foresaw for our system. The majority, 40, anticipate it will evolve as a private, highly-regulated system that rewards competition and innovation. The rest think it’s destined to be a public utility, since it’s highly politicized and widely misunderstood. They acknowledged it’s complicated and admitted to confusion about the Repeal and Replace legislation and the political theatre surrounding it. Their view—that the government plays a necessary role in healthcare in standardizing care, assuring access and equity, and fair play—seems widely held per polls by Pew, Kaiser Family Foundation and others. That’s healthcare! Big. Complex. Expensive. Necessary.
What you need to know is that the American Health Care Act marks the first phase of the GOP’s effort to re-position our health system as an industry empowered by private enterprise and less regulation. What you need to watch is how the new administration and GOP-led Congress implement this shift and the results therefrom.
Secretary Price told NBC’s Meet the Press yesterday that the AHCA will result in "more people covered than are covered right now, and at an average cost that is less." Others think otherwise: Brookings Institution thinks 15 million will lose insurance coverage, Standard and Poor’s believes a loss of 6 to 10 million is more likely and Harvard’s David Cutler estimates the number who lose coverage could reach 20 million. We’ll know soon.
The American Health Care Act is a significant piece of legislation. Be watchful. Like the Affordable Care Act, it’s a big deal.
Paul
P.S. Watch for the Congressional Budget Office’ score for the AHCA and the reactions across the aisle. No doubt, it will prompt media attention especially if it concludes the AHCA will add to the deficit and cover fewer people. Stay tuned!Grammar... The difference between feeling your nuts and feeling you're nuts.Comment
-
Hamtramck is actually Muslim majority.Originally posted by froot loops View Post2012 Detroit Lions Draft: 1) Cordy Glenn G , 2) Brandon Taylor S, 3) Sean Spence olb, 4) Joe Adams WR/KR, 5) Matt McCants OT, 7a) B.J. Coleman QB 7b) Kewshan Martin WRComment
-
One of the things I really miss from living in Detroit is going over for a dinner at Dearborn. Loved the area and restuarants there.Originally posted by hack View Post2012 Detroit Lions Draft: 1) Cordy Glenn G , 2) Brandon Taylor S, 3) Sean Spence olb, 4) Joe Adams WR/KR, 5) Matt McCants OT, 7a) B.J. Coleman QB 7b) Kewshan Martin WRComment
-
CBO predicts current Republican bill will reduce the number of insured by 14 Million by 2018; 24 Million by 2026
Republicans largely expected this which is why they have stressed the importance of ''access" rather than coverage
Comment
Comment